Let’s talk about our kids and the things they put inside themselves. Pediatric foreign body ingestion/insertion is a common emergency room presentation. Maybe it’s just part of them exploring their world. In fact, I recall getting a pearl in my ear and a dime in my nostril as a child; maybe I wanted to start saving at a young age… Bottom line: kids get in trouble. And it’s not always their fault. Families sometimes leave things lying around the house. Children may be fed something they can’t handle. Then there’s always the older sibling putting stuff in them…
More than 100,000 cases of accidental pediatric foreign body ingestion occur each year. I’m going to address the three main orifices where things are placed and let you know the dangers, potential solutions and what to expect if and when you show up in the emergency room. Yep, three different holes, because different types of insertions occur, each with their own risks. I guess they figure if there’s a hole, something needs to go in it.
Ears:
What Happens: Kids will put anything that will fit in their ears, but the problems arise when something either gets stuck or breaks off in an ear. This can include such things as a cotton swab, food, a toy (a bead, something waxy, or something pointy) or whatever else they get their hands on. This poses a significant risk of infection, bleeding and possible rupture of the eardrum, which can lead to an entirely new set of complications.
What You Need to Know: Regardless as to the nature of the item, removal of the item is going to be very dramatic. At home, you should be very conservative in your efforts to get anything out of a child’s ear. Blind efforts may lead to pushing the item further back on the eardrum, possibly rupturing it, or jabbing it into the ear canal, causing damage and potentially setting up an infection. Such efforts usually make it even more difficult for health professionals to get at it once you come to the ER or your doctor’s office.
What happens in the ER: Drama. Depending on the size, shape and depth of the object, tools to flush it out, suck it out, scoop it out or pick it out may be used. There is no guarantee of success, and if the object is unable to be easily retrieved (without an unacceptable risk of further ear damage), the child may either be put to sleep to make the process easier, or you may be referred to an ears, nose and throat specialist.
Nose:
What Happens: Somehow kids think that because of the shape of the nostrils, round things just belong in there. Those smooth pearls, beads, marbles and kernels fit just right.
What You Need to Know: The particular danger with items placed in the nose is they can become dislodged into the airway and choke the child. You should be mindful of this as you try to get that object out yourself. One strategy that you might safely try (assuming no blood or significant pain or other apparent injury exists) is to ‘blow your child a kiss’. Put your mouth around the kids mouth and give a big puff. Sometimes this will pop the object out of the nostril! More easily, if the child is big enough to blow his/her nose, try that while occluding the unaffected nostril.
What Will Happen in the ER: We may try the same things described above. We may also use a piece of equipment called an Ambu-bag to deliver that same type of puff. If that doesn’t work, we have additional means to enter the nose and try to remove the object. The most important consideration is to protect the child’s airway.
Throat to the Stomach or Lower Airway:
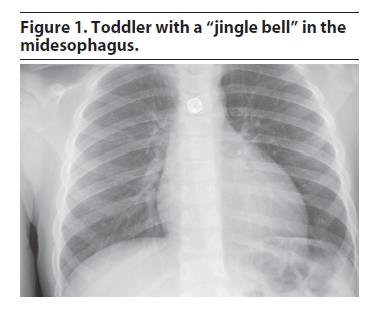
What Happens and What You Need to Know: More foreign object ingestions and aspirations (passage down the airway) occur in children younger than 3 years than in other age groups, although they do occur in all ages. Even relatively immobile infants may get something inappropriate in their mouths despite not being able crawl or pick up objects and put them in the mouth. Their relative inability to chew, coupled with faster breathing rates increases the odds of objects entering the windpipe instead of the food pipe. We see simple things such as nuts, raisins, coins, magnets, seeds, foods (e.g. hot dogs and grapes), as well as toys, pins, batteries, balloons, bones and many other items. Your pediatrician has likely advised you to avoid giving certain foods until the child is at least 5 years old.
Objects that have entered or passed through the throat will leave a sensation that something is still in the throat, particularly if it scratched something on the way down. Objects in the airways run the risk of partial or complete obstruction of different parts of the airway. This can be immediately life-threatening if severe enough obstruction has occurred. There’s no guesswork here; the child will be having difficulty breathing, coughing, gasping and likely turning blue.
What Will Happen in the ER:
Management of swallowed or aspirated foreign body depends on the size of both the object and child and the object’s location.
1) If it’s in the stomach or beyond: unless there are multiple sharp objects that suggest something’s been perforated, little will be done, and you’ll be instructed to wait and watch for it in the stool.
2) If it’s in the airway, this is an emergency, and a lung specialist will need to get the object out with a special scope.
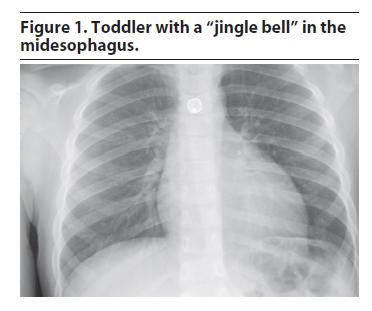
3) If it’s in the food pipe but not yet in the stomach or beyond, what’s done will depend on the size and location. Esophageal foreign bodies (that is, those in the food pipe) generally require early removal by a specialist because of their potential to cause respiratory problems (by manual pressure onto the windpipe) and complications to the esophagus itself (scratches, burns or even rupture). Most notably, ingestion of those annoying button batteries, and their lodging in the esophagus require urgent removal even if no symptoms are present because of an unacceptably high risk of complications. Sharp foreign bodies (except for single straight pins) are especially dangerous and prone to complications and most likely will also need to be removed.
So, after all that, is there any wonder why we ask you to child-proof your home? The dangers are real, and the drama of an ER visit for these things is avoidable and worth being diligent at home. Have a great, safe, healthy and happy weekend.
Thanks for liking and following Straight, No Chaser! This public service provides a sample of what http://www.SterlingMedicalAdvice.com (SMA) will offer beginning November 1. Until then enjoy some our favorite posts and frequently asked questions as well as a daily note explaining the benefits of SMA membership. Please share our page with your Friends on WordPress, and we can be found on Facebook at SterlingMedicalAdvice.com and on Twitter at @asksterlingmd.
Copyright © 2013 · Sterling Initiatives, LLC · Powered by WordPress