It would be improper for me to have dragged you through the mud for three days and depressed you into thinking you can’t improve your situation. Hopefully, you’re not feeling that way. You should now have a better understanding of how the body works, how to count calories and how to compare yourself to a baseline for health. What left is giving your body a leg up on your efforts. Yep, I’m talking about boosting your metabolism. Any of you that have been with me for a while know that means I’m not promoting something you’ll find in a bottle, although there are many good supplements that can assist in that effort. I’ll refer you to your (or my) favorite personal trainer for those considerations. As always, I want to offer you the tools to be self-empowered. To that end, here’s five Quick Tips to boost your metabolism. Why five? Because five is easier to implement than six. Once you get these five down, let me know, and we can get a bit more intricate.
1. Eat smaller meals, and eat more frequently. It’s true. More meals more often is better, but only if they’re smaller. Calorie counting is still a major part of the equation. The point of more frequent meals is preventing the body from going into starvation mode, which slows your metabolism as the body attempts to conserve energy. If you do this, you’ll discover those meals are smaller and you will get closer to eat more appropriate portions than we typically do. Also, make those in-between meals healthy choices like a handful of fruits or nuts.
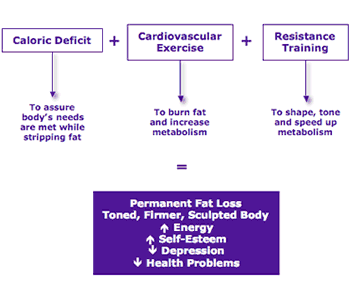
2. Prime your pump. Remember, it’s all about your heart’s ability to efficiently move blood around the body anyway. The healthier your heart is, the better your metabolism will be. You need aerobic exercise that increases your heart rate for 20-30 minutes at a time. Learn your target heart rate for your age, and exercise to get into that range. Your metabolism will better approximate that of a fine tuned machine rather than a sputtering old car.
3. Weight train. This is very simple. The more muscular you are, the more calories you will burn, especially relative to someone of the same weight who is obese. Not only will you become a finer calorie-burning machine, in this case you actually will look better! Add weight training to your exercise regimen.
4. Choose the fish (and not the fried variety). Fish oil contains substances called omega-3 fatty acids (EPA, DHA) which increases levels of fat-burning enzymes and decreases levels of fat storing enzymes. Daily ingestion has been shown to help by approximately 400 calories a day.
5. Enlist a personal trainer. Everyone needs help and motivation. Some of us need a lot of help and a lot of motivation. We also need expertise. There’s nothing more frustrating than working hard yet not seeing any results because you’re working incorrectly. A good trainer can put you on the path, supervise your regimen, and hold your hand through the process. The minutia of age, sex and body habitus considerations that also play a role in this can be managed by a good trainer. Your ideal trainer will have knowledge of nutrition, wellness and supplements that are tailored to your specific considerations. This will get your metabolism revved up!
By the way, if you’re into green tea, caffeine or spicy/hot peppers, enjoy them for their other benefits, but don’t expect them to contribute significantly to your efforts to improve your metabolism. At least that’s what the consensus in the medical literature points out.

Finally: yes, it’s true that metabolism naturally slows with age (starting as early as age 25); everyone has heard that fact. However, here’s what you don’t usually hear: that’s not inevitable and is more a result of your becoming less physically active than just aging. That demonstrates the need for you to be even more diligent in your efforts. Good luck, and I welcome your questions and comments.
















































![exercize cat[5]](https://jeffreysterlingmd.com/wp-content/uploads/2014/05/exercize-cat5.jpg)







{kind=link}