Every so often, controversies regarding medical treatment recommendations get in the news and seemingly only serve to confuse the public. Every blog, article or research paper is a single entity that may or may not adjust the body and weight of evidence on a given topic. Even most well-done research articles do not completely change the standard of care for medical practice. Prostate cancer screening is a great example. At the end of it all, controversies aren’t as important as the consensus recommendations that emerge from medical and public health professionals tasked with reviewing such information.
In this Straight, No Chaser, we will review the 2015 recommendations from the American Cancer Society (ACS) for early detection of prostate cancer. Remember, when you hear dissenting views, consider the source and balance that against the formal recommendations of ACS.
In an earlier Straight, No Chaser, several questions regarding prostate cancer were addressed. However, there is one additional question that is important to review.
Does Everyone With Prostate Cancer Get Treated?
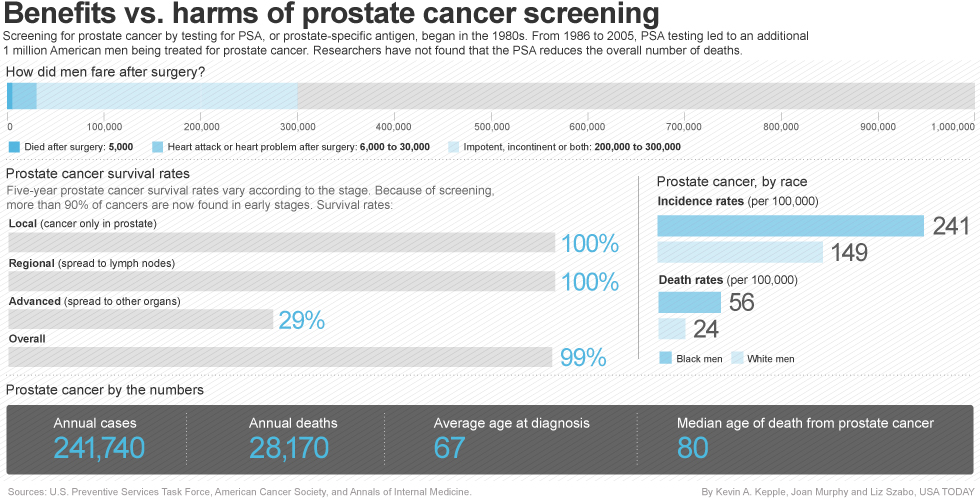
This is the source of controversies regarding screening of prostate cancer. Most men diagnosed with prostate cancer do not die from the disease. I mentioned previously that 30,000 men with prostate cancer die of the disease every year. However, over 2.5 million men in the U.S. are currently living with a diagnosis of prostate cancer. Based on these statistics, the question then becomes…
Why Do All Men Need to Be Screened For Prostate Cancer?
A certain stream of logic asks why screening is necessary if most of those who are diagnosed don’t die. Many treatments (e.g. surgery, medications, radiation) have additional risks that could be avoided if interventions were avoided. Similarly, some have taken to asking if any screening program is necessary. The view here is information is empowering. It’s always better to have information regarding the state of your health. Working with your medical team and family, the correct decisions about next steps can be made. This option is only available if you know what’s happening with your health.
How Does Screening Occur?
There are two tests commonly used to screen for prostate cancer.
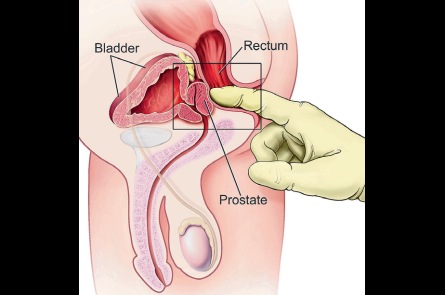
- A digital rectal exam (DRE) is when a doctor inserts a gloved, lubricated finger into the rectum and estimates the size of the prostate and assesses it for lumps or other abnormalities.
- The prostate specific antigen (PSA) test measures the level of PSA in the blood. PSA is a substance made by the prostate, and PSA blood levels can be higher in men who have prostate cancer. Unfortunately the PSA level isn’t specific for prostate cancer, as it can be elevated in other conditions that affect the prostate such as age, race, certain medications or medical procedures, prostate enlargement or infection.
So What Are The Current Recommendations for screening?
The American Cancer Society (ACS) recommends that men get to decide if they want to be screened, based on a recommendation from their physician and having received information about the risks, benefits and uncertainties surrounding screening. In other words, we don’t even talk about screening anymore; now it’s “Who should have a conversation with their physician about getting screened?”
- If you’re age 50 and have an average risk of prostate cancer and are expected to live at least 10 more years. Because prostate cancer grows slowly, if your life expectancy is less than 10 years, you wouldn’t benefit from screening or treatment for prostate cancer.
- If you’re age 45 for men and are at high risk of developing prostate cancer. This includes African-Americans and men who have a first-degree relative (father, brother, or son) diagnosed with prostate cancer at an early age (younger than age 65).
- If you’re age 40 for men at even higher risk (those with more than one first-degree relative who had prostate cancer at an early age).
Among these groups, when the decision is made to screen, those men will be tested with the prostate-specific antigen (PSA) blood test. The digital rectal exam (DRE) may also be done as a part of screening.
Assuming no prostate cancer is found as a result of screening, the need for future screenings depends on the results of the PSA blood test:
- Men who choose to be tested who have a PSA of less than 2.5 ng/ml, may only need to be retested every 2 years.
- Screening should be done yearly for men whose PSA level is 2.5 ng/ml or higher.
Even after a decision about testing has been made, the discussion about the pros and cons of testing should be repeated as new information about the benefits and risks of testing becomes available. Further discussions are also needed to take into account changes in the patient’s health, values, and preferences. Please at least have the conversation with your physician.
Order your copy of Dr. Sterling’s new book Behind The Curtain: A Peek at Life from within the ER at jeffreysterlingbooks.com, iTunes, Amazon, Barnes and Nobles and wherever books are sold.
Thanks for liking and following Straight, No Chaser! This public service provides a sample of what http://www.SterlingMedicalAdvice.com (SMA) and 844-SMA-TALK offers. Please share our page with your friends on WordPress, like us on Facebook @ SterlingMedicalAdvice.com and follow us on Twitter at @asksterlingmd.
Copyright, Sterling Initiatives, LLC. 2013-2015